
- Mon - Sat 9:00am - 9:00pm
- Sun 9:00am - 2:00pm
- No 218, South Service Road, Phase1,
- Sathuvachari, Vallalar, Vellore - 632009
- Landmark: Near Vallalar Bus Stop
Newborn Surgery

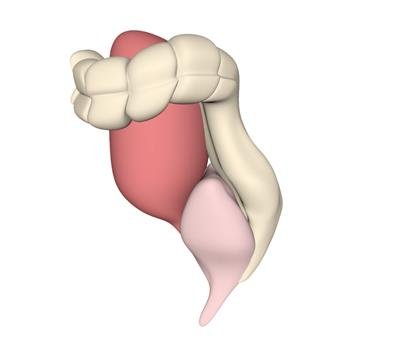
Intestinal Atresia / Duplications
An atresia is a congenital defect of a hollow viscus that results in complete obstruction of the lumen. Intestinal atresia is one of the most frequent causes of bowel obstruction in the newborn and can occur at any point in the gastrointestinal tract. Approximately one-half of the cases involve the duodenum. The outcome of intestinal atresia following surgical repair is very good. In general, morbidity and mortality depend upon associated medical conditions such as prematurity or cystic fibrosis, other congenital anomalies, the complexity of the lesion, and surgical complications. Intestinal duplications, like foregut duplications, are directly contiguous with the segment from which they are associated. Duplications are dorsal to the intestine, usually mesenteric and sometimes intramural.
Intestinal duplications are uncommon, occurring in just 1 in 10,000 live births. Males appear to be more commonly affected (60 to 80% of cases). About one third of affected children have associated congenital anomalies. The etiology of intestinal duplications is unknown. Theories include abnormalities in recanalization, a vascular insult, persistence of embryonic diverticula, and partial twinning. The most common site of duplication is the jejunum and ileum followed by the colon, stomach, duodenum, and esophagus. Colonic duplication is often associated with anomalies of the urogenital system. Intestinal duplications usually manifest in the 1st or 2nd year of life.

Anorectal Malformations
Anorectal malformations are birth defects, or problems that happen as an unborn baby is developing during pregnancy. With this defect, the anus and rectum don’t develop properly. They are the lower part of the digestive tract. Normally during a bowel movement, stool passes from the large intestine to the rectum and then to the anus. Muscles in the anal area help to control when you have a bowel movement. Nerves in the area help the muscles sense the need for a bowel movement. The nerves also stimulate muscle activity. As an unborn baby is growing in its mother's womb or uterus, different organ systems are developing and maturing. The lower end of the intestinal tract forms fairly early in pregnancy. In an unborn baby, the lower part of the large intestine and the urinary tract start off as one large mass of cells. Certain steps must happen in the first 3 months of pregnancy or gestation. These steps are needed for the rectum and anus to break away from the urinary tract and form properly.
Hirschsprungs Disease
Hirschsprung's (HIRSH-sproongz) disease is a condition that affects the large intestine (colon) and causes problems with passing stool. The condition is present at birth (congenital) as a result of missing nerve cells in the muscles of the baby's colon. A newborn who has Hirschsprung's disease usually can't have a bowel movement in the days after birth. In mild cases, the condition might not be detected until later in childhood. Uncommonly, Hirschsprung's disease is first diagnosed in adults. Hirschsprung disease is a birth defect in which nerve cells are missing at the end of a child’s bowel. Normally, the bowel contains many nerve cells all along its length that control how the bowel works.

Mesenteric Cysts
Mesenteric cysts most commonly occur in the small-bowel mesentery on the mesenteric side of the bowel. They can often be shelled out from between the leaves of the mesentery with care taken to avoid damage to the mesenteric vessels, or they may require concomitant bowel resection in order to ensure that the blood supply to the bowel is not compromised. Rare condition of the mesentery and omentum due abnormal blockage of lymphatic drainage leading to the formation of fluid filled structures called cysts. Double layer of tissue connecting the small intestines to the rest of the body. This is where the blood vessels to the intestines are located. Mesocolon is the mesentery to the colon. These masses can be incidental findings on CT scans or during abdominal operations for unrelated conditions. Patient complaints are nonspecific. Children with symptoms can have abdominal distention due to enlarging cyst or vague abdominal pain with or without a mass. Sometimes symptoms can mimic intestinal blockage or appendicitis.

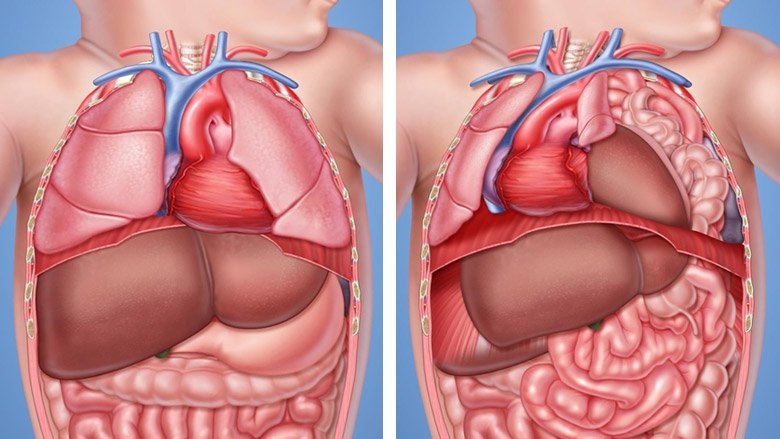
Diaphragmatic Hernia
A diaphragmatic hernia is a birth defect in which there is an abnormal opening in the diaphragm. The diaphragm is the muscle between the chest and abdomen that helps you breathe. The opening allows part of the organs from the belly to move into the chest cavity near the lungs. A diaphragmatic hernia is a rare defect. It occurs while the baby is developing in the womb. The diaphragm is not fully developed. Due to this, organs, such as the stomach, small intestine, spleen, part of the liver, and the kidney may take up part of the chest cavity. CDH most often involves only one side of the diaphragm. It is more common on the left side. Often, the lung tissue and blood vessels in the area do not develop normally either.
CLE / CCAM - Lung Disorders
Congenital lobar emphysema (CLE), also known as congenital lobar overdistension, is a usually postnatally diagnosed malformation of the lung, which can be characterized by air trapping and overdistension of segments and lobes. In some cases, there is respiratory distress, a mediastinal shift, and wheezing due to spontaneous overinflation of the affected areas. Prenatal diagnosis has been made in a number of cases but in most cases, the diagnosis was made postnatally. Such fetuses have a congenital echogenic mass, including a mediastinal shift and displacement of the heart, resulting in compression of the contralateral lung. Also, macrocystic and microcystic lesions have been reported. In a series of 94 cases of congenital masses of the lung, it was only possible to make the correct diagnosis of CLE in 6 patients after birth. This condition is diagnosed at birth in about 25% and at the age of 1 month in about 50%. The diagnosis is sporadic after 6 months. Standard treatment for the acute neonatal respiratory distress in this diagnosis is surgical removal of the affected lung area. In some cases of neonatal respiratory distress, however, there is spontaneous resolution.